

缺牙很痛苦 雖然可以戴活動假牙
但很不好用 大大影響生活品質
如下圖 全口缺牙的患者 活動假牙直接壓在牙肉上
沒甚麼固著力 假牙易鬆脫


所以早在1910年代 就想出一些辦法 來解決缺牙的痛苦
開始出現”植牙”的概念
想盡辦法 讓”活動”假牙 變成”固定”假牙
因此設計出 各種不同的金屬架構 來”固定”假牙
…….
最早 1913年 Greenfild 就提出以金屬為材料
做成”籃狀”植體(hollow basket) 埋入骨內 來支撐假牙的構想…

1940 以後 植體種類 大致分為三類
Subperiosteal Implant (骨膜下植體)
Transosseous Implant (穿骨植體)
Endosseous Implant (骨內植體)
Subperiosteal Implant(骨膜下植體)
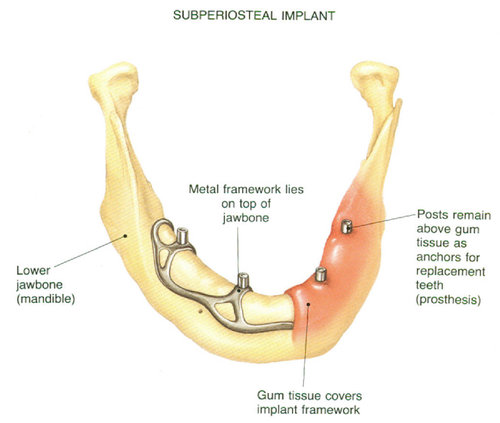
1940年代 由Dahl, Goidberg&Gershkoff 所提出發展而來
主要是針對全口無牙的病患(Totally edentulous mandible & maxilla)所設計
全口無牙的患者 配戴活動假牙時 因沒有固著 假牙容易”鬆脫”
所以他們就想以手術方式 在顎骨上 加上一個金屬架 以”抓住”活動假牙
多用在顎骨嚴重萎縮 (advanced bone loss )的患者
以鈷-鉻-鉬(C0-Cr-Mo)或氧化鋁(Aluminum oxide)為材料
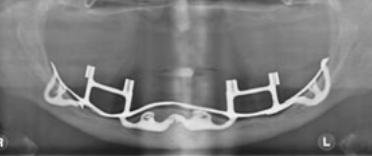
做成支架 跨在顎骨上 以骨膜包覆之(所以稱為”骨膜下植體”)
作為支撐假牙的金屬架
但效果並不好 支撐力道不盡理想
術後腫脹發炎較嚴重
戴上假牙後 疼痛比例高 (Post-insertion Dysesthesia)
而且容易造成下齒槽神經的撕裂(Laceration of the mandibular nerve)
成功率較低 所以現在比較少有人用此方法來重建咬合
有興趣的人 可參考2007 德國Zwerger S 等人所發表的相關文章…
[Long-term results of fittig subperiosteal implants: report of twelve patient cases].
Zwerger S, Abu-Id MH, Kreusch T.
Source
Asklepios Klinik Nord, Heidberg, Mund-, Kiefer- und Gesichtschirurgie, Tangstedter Landstr. 400, Hamburg 22417, Germany. stefan.zwerger@k-nord.lbk-hh.de
Abstract
The subperiosteal dental implantation implant was orginally described in the 1940s. The inadequate long-term results of subperiosteal implants are in contrast to the excellent results documented for endosseus oral implants. Consequently, subperiosteal implants and other soft-tissue-anchored implants should not be used presently. The present report documented twelve patient cases with complications after treatment with subperiosteal implants. Typical complications of SI are implant exposure, inflammation, infection, fistula formation and implant mobility. After removing the SI severe atrophic bone was seen. The placement of osseointegrated oral implants was mostly not possible without autogenous bone grafting. The present report is in conclusion with other studies, that a regular control of patients with subperiosteal implants is necessary. Subperiosteal implants should definitely be removed, if continuous periods of complication occur. The complete oral rehabilitation requires further surgical treatment in the field of preprosthetic surgery.
Transosseous Implant(穿骨植體)

由1975年 Dr. Small 所發展出來
以Co-Cr-Mo或Au 為材料 做一個支架
以外科手術方式 所在下顎骨上(如下圖)
此方法只適用於下顎
需全身麻醉 手術範圍大
須由口外開刀進入 會在下巴留下傷痕
骨喪失大 易感染
費用很高 較不經濟
這種方式因該沒有多少人願意嘗試吧
Endoesseous Implant (骨內植體)

顧名思義 就是將植體埋入骨頭里
因為”骨整合”的發現 骨頭會跟鈦金屬緊密結合
所以將鈦金屬埋入骨頭裡面 會得到很好的固著效果
強大的固著力 就可以來支撐咬合壓力
植體的形狀不同 又分為
刀型植體(Blade-Vent type)

柱狀植體(Cylinder type)

螺紋植體(Screw type)

早期Blade-Vent type 由Linkow(1966), Roberts&Roberts(1970) 所發展出來
以Co-Ni-Va, Vitreous carbon 為材料 用於齒槽骨很窄(narrow ridge)的case
但缺乏骨整合及力學的基礎 容易有持續性的骨破壞(continuous bone loss)
目前已少有人使用
現今大部分的植體多採用”螺紋植體”(Screw type implant)
它的基本型態設計 是由瑞典醫師Dr.Branemark於70年代所提出
其中一些基本設計 還一直沿用至今
成為目前植體設計基本架構的主流 !
在臨床這麼多年
只有看過兩三次刀型植體在患者口中
很興奮 趕快記錄下來
不過要把它拆下來 沒有想像的容易
花了好大功夫
病人也受累不少
現代植牙 經過半個多世紀的發展
已成熟許多 比以前幸福多了
輕鬆愉快 沒那麼恐怖 !!
不過還是好好定期洗牙保養
畢竟自己的牙齒比植牙更好
天然的尚好 ~